
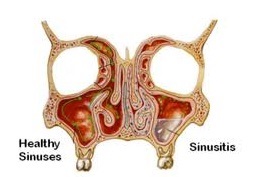
The most important element in development of sinusitis is the osteomeatal complex consisting of the outflow tracts of all of the sinuses into the nose. The cilia move mucus toward the naturally occurring ostium. If the cilia are interfered with, stagnation of mucus will occur. In situations where the ostia are obstructed, such as with inflammation, viruses, allergic rhinitis, foreign bodies, and polyps, mucociliary clearance will be impaired. The reduction in patency of the ostium typically will cause a reduction in oxygen content within the sinuses, increasing the likelihood of bacterial overgrowth.
A change in air pressure inside the sinuses will cause localized pain. This can occur both from obstruction of the ostia and increased mucus production, as well as a change in air pressure such as with flying or diving. For this reason acute treatment is more important prior to such activities.
A clinical history of the patient will be created before any surgery is performed. A careful diagnostic workup is necessary to identify the underlying cause of acute or chronic sinusitis. This may necessitate a paranasal sinus CT scan, nasal endoscopy, rhinomanometry and selected blood tests to determine an operative strategy. Note: Sinus X–rays have limited utility in the diagnosis of acute sinusitis and are of no value in the evaluation of chronic sinusitis.
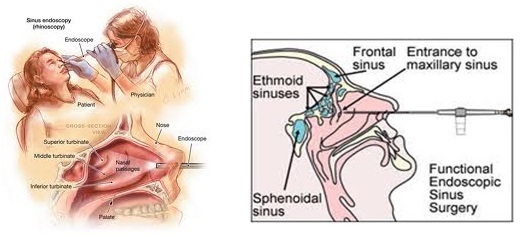
Functional endoscopic sinus surgery (FESS): The use of an endoscope is linked to the theory that the best way to obtain normal healthy sinuses is to open the natural pathways to the sinuses. Once an improved drainage system is achieved, the diseased sinus mucosa has an opportunity to return to normal.
FESS involves the insertion of the endoscope into the nose for a direct visual examination of the openings into the sinuses. Abnormal and obstructive tissues are then removed by endoscopic instruments. In the majority of cases, the surgical procedure is performed entirely through the nostrils, leaving no external scars.
The advantage of the procedure is that the surgery is less extensive; there is often less removal of normal tissues. Nowadays, most of the cases do not require nasal packing even after surgery. After the operation, the patient, if required, will have nasal packing for 24 to 48 hours. Ten days after the procedure, nasal irrigation may be recommended to prevent crusting and regular follow up visits to check endoscopically.